

Abstract
Introduction: A diagnosis of multiple myeloma (MM) has a substantial impact on health-related quality of life (HRQoL) due to associated symptoms, such as bone pain, infection, and fatigue. Furthermore, HRQoL deteriorates with each subsequent line of therapy. The phase 3 OPTIMISMM study (NCT01734928) demonstrated that pomalidomide, bortezomib, and low-dose dexamethasone (PVd) resulted in a significantly longer progression-free survival (PFS) and greater overall response rate (ORR) compared with bortezomib and low-dose dexamethasone (Vd) in patients with relapsed or refractory multiple myeloma (RRMM), all of whom had received prior treatment with lenalidomide. Given that HRQoL in RRMM is an important consideration, we conducted this analysis to evaluate the effect of PVd versus Vd on HRQoL in patients enrolled in the OPTIMISMM study.
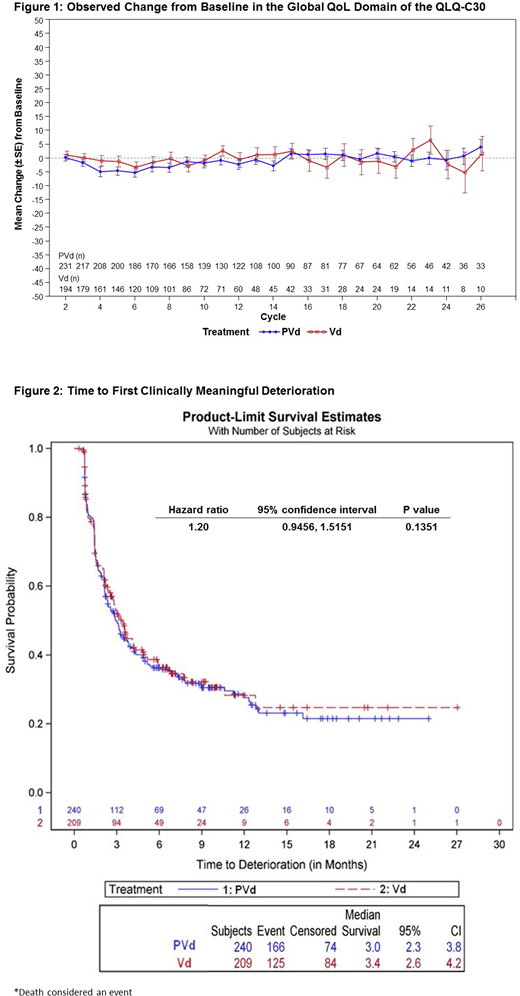
Methods: The OPTIMISMM study was a phase 3, multicenter, randomized, open-label study that enrolled adult RRMM patients who had received 1 to 3 prior anti-myeloma regimens including lenalidomide. Patients (N=559) were randomly assigned to receive PVd (n=281) or Vd (n=278) per 21-day treatment cycle until progression or treatment discontinuation. HRQoL was assessed as an exploratory endpoint using the European Organization for Research and Treatment of Cancer (EORTC) Quality of Life Core 30 (QLQ-C30) questionnaire at Day 1 of each 21-day cycle prior to treatment administration and at the end of treatment. The primary domain of interest was the Global Health Status/QoL domain of the QLQ-C30. Analyses were performed in the HRQoL-evaluable population, which included randomized patients who completed the QLQ-C30 assessment at baseline and at least one post-baseline visit. Key primary analyses of PVd versus Vd on the global QoL domain of the QLQ-C30 included a longitudinal assessment of change from baseline using a mixed-model repeated measure (MMRM) approach; an assessment of the proportion of patients experiencing clinically meaningful deterioration (i.e., ≥10 points worsening from baseline) at pre-selected post-baseline visits; and an analysis of time to first clinically meaningful deterioration.
Results: The HRQoL-evaluable population consisted of 240 patients in the PVd group and 209 in the Vd group; baseline characteristics were well-balanced between the treatment groups. HRQoL compliance rates based on the number of patients expected to complete the QLQ-C30 at each given visit exceeded 80% for most visits among both groups. Mean (SD) baseline scores for the global QoL domain of the QLQ-C30 were similar between groups (61.0 [23.2] in the PVd group and 63.5 [21.3] in the Vd group); these scores were maintained over time for both treatment groups, with no clinically meaningful differences observed between the treatment groups at any cycle (Figure 1). The MMRM analyses showed no clinically meaningful difference in global QoL of patients between the PVd group and the Vd group. There was also no significant difference observed in the proportion of patients who experienced clinically meaningful worsening in the global QoL domain between the treatment groups throughout the pre-selected post-baseline visits. The median time to the first clinically meaningful worsening was also similar between treatment groups: 3.0 months for the PVd group and 3.4 months for the Vd group, respectively (hazard ratio: 1.20; 95% confidence interval: 0.9456, 1.5151; p=0.1351; Figure 2 for when death was considered as an event); similar results were observed when death was censored.
Conclusions: The results from this analysis of the OPTIMISMM study showed that the triplet regimen of PVd, which consisted of pomalidomide added to the doublet regimen of Vd, did not compromise HRQoL in lenalidomide-treated patients with RRMM. Overall, there were no clinically meaningful differences in the Global Health Status/QoL domain of the QLQ-C30 between treatment groups. These results are meaningful and provide further evidence of the clinical benefits of the addition of pomalidomide to Vd, which include significant improvements in PFS and ORR.
Weisel:Amgen, BMS, Celgene, Janssen, Juno, Sanofi, and Takeda: Consultancy, Membership on an entity's Board of Directors or advisory committees; Amgen, Celgene, Janssen, and Sanofi: Research Funding; Amgen, BMS, Celgene, Janssen, and Takeda: Honoraria. Dimopoulos:Takeda: Honoraria; Bristol-Myers Squibb: Honoraria; Amgen: Honoraria; Janssen: Honoraria; Celgene: Honoraria. Moreau:Amgen: Honoraria, Membership on an entity's Board of Directors or advisory committees; Takeda: Honoraria, Membership on an entity's Board of Directors or advisory committees; Celgene: Honoraria, Membership on an entity's Board of Directors or advisory committees; Janssen: Honoraria, Membership on an entity's Board of Directors or advisory committees; Abbvie: Honoraria, Membership on an entity's Board of Directors or advisory committees. Larocca:Amgen: Honoraria; Bristol-Myers Squibb: Honoraria; Celgene: Honoraria; Janssen-Cilag: Honoraria. Rodriguez Otero:Clínica Universidad de Navarra: Employment; Takeda: Consultancy; Bristol Myers Squibb: Research Funding; Celgene: Consultancy, Honoraria, Research Funding; Janssen: Consultancy, Honoraria. Anttila:Janssen: Membership on an entity's Board of Directors or advisory committees; Amgen: Membership on an entity's Board of Directors or advisory committees; Takeda: Consultancy, Membership on an entity's Board of Directors or advisory committees. Hayden:Celgene: Honoraria; Jassen: Honoraria; Amgen: Honoraria. Krauth:Celgene: Consultancy, Honoraria; BMS: Consultancy, Honoraria; Novartis: Consultancy, Honoraria; Janssen: Consultancy, Honoraria; Takeda: Consultancy, Honoraria; Amgen: Consultancy, Honoraria. Guo:Celgene Corporation: Consultancy. Purnomo:Celgene: Employment. Yu:Celgene: Employment, Equity Ownership. Grote:Celgene: Employment. Biyukov:Celgene Corporation: Employment, Equity Ownership. Zaki:Celgene Corporation: Employment, Equity Ownership. Richardson:Karyopharm: Membership on an entity's Board of Directors or advisory committees; Celgene: Membership on an entity's Board of Directors or advisory committees, Research Funding; BMS: Research Funding; Amgen: Membership on an entity's Board of Directors or advisory committees; Takeda: Membership on an entity's Board of Directors or advisory committees, Research Funding; Oncopeptides: Membership on an entity's Board of Directors or advisory committees; Jazz Pharmaceuticals: Membership on an entity's Board of Directors or advisory committees, Research Funding; Janssen: Membership on an entity's Board of Directors or advisory committees.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal